 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
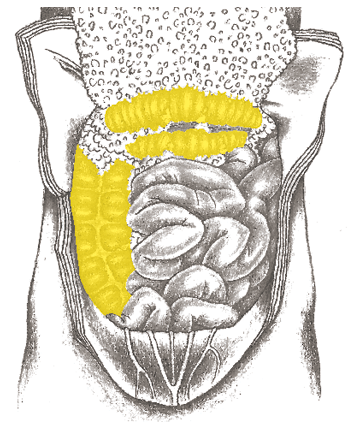
LARGE INTESTINE – ASCENDING, TRANSVERSE, AND DESCENDING
The large intestine (colon) has a diameter of about 6 cm (2 in) and is about 1.5 m (5 ft) long. Unlike the small intestine, the colon has no villi. Nutritional elements and fluid are removed from the food pulp here.
Appendix Mucosa
(not pictured)
Chunk conflict of
the reserves being
in danger
Colon Mucosa
Indigestible-anger
Sigmoid Colon Mucosa
(not pictured)
Indigestible-anger,
not being able to
eliminate something
SBS of the Colon Mucosa
Colon cancer, polyps1
| Conflict | Chunk conflict (see explanations p. 15, 16): indigestible-anger. A situation that is ugly and hard to deal with. |
|---|---|
| Examples | ➜ Something unpleasant, not being able to get rid of “crap.” ➜ Not being able to cope with something vile, devious or mean.  For many years, a man has been a founding member of an organization. A huge argument breaks out among the members because the man who owns the restaurant where they meet no longer wants the meetings to be held there. > Indigestible–anger. A few weeks later, the patient is diagnosed with colon cancer = active–phase. The tumor is surgically removed. Afterwards, he learns about the 5 Biological Laws of Nature. (Archive B. Eybl) A 43-year-old, married, department head uses a friendly approach with her colleagues. Four years ago, a new colleague joins the team. From the very beginning, she works against the department leader. A month ago, she learns that this colleague has been maligning her in the company behind her back. = Indigestible–anger conflict and an “attack-to-the-abdomen” conflict. A month later, the patient speaks of the matter, choosing two close colleagues and a girlfriend to confide in. She starts to feel better during the conversation = conflict resolution. Then, at night, she suffers an intestinal colic (= repair phase crisis) with a hard, swollen abdomen and sweating. It’s so bad that she calls an ambulance. In the hospital, she is diagnosed with an inflammation of the colon and a thickening of the intestinal wall (= flat-growing tumor of absorptive quality). In addition to this, fluid has accumulated in the peritoneal (abdominal) cavity (ascites) and her blood sedimentation levels are high (indication of inflammation), which according to CM “cannot possibly come from the intestines alone“ = peritonitis – resolved attack conflict. After a few days, everything is all right again. (Archive B. Eybl) For many years, a man has been a founding member of an organization. A huge argument breaks out among the members because the man who owns the restaurant where they meet no longer wants the meetings to be held there. > Indigestible–anger. A few weeks later, the patient is diagnosed with colon cancer = active–phase. The tumor is surgically removed. Afterwards, he learns about the 5 Biological Laws of Nature. (Archive B. Eybl) A 43-year-old, married, department head uses a friendly approach with her colleagues. Four years ago, a new colleague joins the team. From the very beginning, she works against the department leader. A month ago, she learns that this colleague has been maligning her in the company behind her back. = Indigestible–anger conflict and an “attack-to-the-abdomen” conflict. A month later, the patient speaks of the matter, choosing two close colleagues and a girlfriend to confide in. She starts to feel better during the conversation = conflict resolution. Then, at night, she suffers an intestinal colic (= repair phase crisis) with a hard, swollen abdomen and sweating. It’s so bad that she calls an ambulance. In the hospital, she is diagnosed with an inflammation of the colon and a thickening of the intestinal wall (= flat-growing tumor of absorptive quality). In addition to this, fluid has accumulated in the peritoneal (abdominal) cavity (ascites) and her blood sedimentation levels are high (indication of inflammation), which according to CM “cannot possibly come from the intestines alone“ = peritonitis – resolved attack conflict. After a few days, everything is all right again. (Archive B. Eybl)• An athletic, 50-year-old entrepreneur has a construction company and his business is booming. Suddenly, this good fortune abandons him: A major customer goes bankrupt and he loses a lot of money. Shortly thereafter, another customer refuses to pay 20% of the agreed fee. = Indigestible-anger conflict. Since then, problems with business partners are always a trigger for him. The result is a chronic inflammation of the colon (ulcerative colitis). After retirement, the disease heals almost completely. (Archive B. Eybl) |
| Conflict-active | Conflict–active Increased function. Growth of a cauliflower-like adeno-ca of secretory quality with a conflict aspect of not being able to digest something or a flat-growing adeno-ca = “tumorous thickening of the intestinal wall“ of absorptive quality with a conflict aspect of not being able to accept something. |
| Bio. function | With more cells in the colon, better ability to digest or absorb the lodged chunk of anger. |
| Repair phase | Normalization of function, tubercular, caseating, necrotizing degradation of the tumor via acid-resistant fungi and bacteria (mycobacteria), mild fever, night sweats, colitis, ulcerous colitis. If bacteria not present: encapsulation. Bright–red blood and mucus in stool, diarrhea. |
| Repair crisis | Chills, heavy bleeding, and colicky pain. |
| Questions | First, determine if it is an active or a resolved conflict. (Questions about the symptoms, look at the inflammation levels in the blood). Estimate the length of the conflict based on the size. What was I unable to digest over the period in question? What has been pressuring me for a long time? What issue is hard for me to talk about (isolation)? What “crap” would I like to be rid of? Which conditioning is in the background of the conflict? Which new attitude and which external changes would heal me? |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life if they are still active. Guiding principles: “Nobody profits from anger.“ “Everything has a purpose and I can only learn from this.“ Surgery if the passage is obstructed or the polyp/tumor is too large. If you are going to have an OP, earlier is better than later, because small tumors are often diagnosed as “benign” by CM today CM. > I.e., less stress for the person concerned. See also: remedies for the colon, p. 255. |
Intestinal obstruction (ileus)
This diagnosis can mean an obstruction due to a tumor or paralysis of the intestinal musculature (paralytic ileus). See SBS of the intestinal muscles p. 243. With paralytic ileus, no tumor is found during a colonoscopy. If a tumor is the cause: same SBS as above (see above).
| Phase | Conflict–active: an intestinal occlusion occurs when the tumor is too big or often at the beginning of the repair phase due to the inflammation-swelling of the tumor. |
|---|---|
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life if they are still active. Questions: see: p.246. Surgery if necessary. |
Chronic inflammation of the intestines (Crohn‘s disease, colitis ulcerosa)2
Same SBS as above. (See pp. 245.) In CM, the difference between Crohn‘s disease and colitis ulcerosa is vague; the differentiation is also unnecessary. If the small intestine is also affected, a starvation conflict is also underway (see: p. 196).
| Examples | A man is constantly angry and arguing with his wife = indigestible–anger. He would have separated from her long ago if it were not for their house, which he would lose in a divorce. The conflict has been growing now for two decades = recurring–conflict. The patient suffers from a severe case of Crohn‘s disease. (Archive B. Eybl) The schoolboy feels he is being treated unfairly by his teacher. He thinks that she always grades him worse than he deserves. Diagnosis: Crohn‘s disease due to recurrences. (Archive B. Eybl) |
|---|---|
| Phase | Chronic-recurring process. Active-phases alternate with repair phases. Flat-growing adeno-ca of resorptive quality, sometimes polyps as well (secretory quality). Blood, mucus in the stool. Diarrhea, constipation, and night sweats. |
| Therapy | Determine the conflict and triggers and, if possible, resolve them in real life, so that the SBS comes to an end. Questions: see above. Guiding principles: see above. Good chances of recovery, even with long-standing cases. See also: remedies for the colon, p. 255. Questions: see: p.246. The CM therapy with cortisone, immunosuppressants, and anti-TNF agents is not recommended over a prolonged period. |
Testimonials
All experience reports on the organ system „Large Intestine – Ascending, Transverse, and Descending” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2025/12/11   Myocardial infarction following a resolved overwhelming conflict due to poorly made dentures. | Overwhelming conflict, indigestible conflict, territorial-anger conflict | ||||
 | 2025/10/21 Chunk conflict: healing of ulcerative colitis (medically confirmed) by clarifying the conflict and the family imprint | Chunk conflict, ulcerative colitis | ||||
2025/03/24 This documentary presents 15 individuals who were diagnosed with cancer by conventional medicine and who examined the causes of their symptoms according to the model of the so-called 5 Biological Laws of Nature and overcame them.  | Colon cancer, bone cancer, breast cancer, skin cancer, testicular cancer, pancreatic cancer, cervical cancer | |||||
 | 2025/03/05 A man of Turkish descent has been living in a completely Islamic environment within a socially European country for four years with a diagnosis of ulcerative colitis. The conflict arises from the transition between these worlds under the emotional pressure of the Islamic world (mainly family). The conflict has been resolved—the medication has been discontinued.  | |||||
2025/02/07 The dirt, the underhandedness or smut that she couldn't get rid of was the bad domestic situation with her husband. He was showing more and more interest in the female guests at her boarding house. As the situation escalated, he became violent towards her, saying: “If you think you can run away, I guarantee you won't survive!” This terrible situation resulted in the growth of the colon mucosa, as well as other things.  | Colon cancer | |||||
 | 2024/10/07 Mainstream medicine considers Irritable Bowel Syndrome (IBS) a chronic condition that requires lifelong management and treatment to control symptoms. Emotional Freedom Techniques (EFT) focus on addressing the underlying emotional issues, aiming for permanent results rather than just symptom management. This case study demonstrates the steps taken to resolve 'lifelong' IBS symptoms using EFT exclusively. | Case Report, EFT, IBS, Irritable Bowel Syndrome, Chronic Disease, EFT Approach, Chronic Physical Symptoms | ||||
 | 2023/09/10 How the threat and implementation of a really long period of lockdown led to menstrual pain, paralysis and diarrhea. | Menstrual pain, movement paralysis, diarrhea, chronic process | ||||
 | 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. | |||||
 | 2014/12/29 October 22nd of this year I suddenly had very liquid stool. I wasn't irritated at first because this can always happen, but it didn't stop ... |