 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
PENIS AND URETHRA
Basically, the penis can be divided into root, penile shaft and the glans penis. The mesodermal cavernous bodies (two larger ones on the side and a smaller one below containing the urethra) cause erection.
The foreskin (preputium) constitutes a doubling of the shaft skin in the form of two leaves of skin. The inner leaf holds endodermal glands, which produce a sebaceous lubricant (smegma). The penile shaft and glans penis are covered with ectodermal squamous epithelium, as well as the urethra (urothelium).
Penile Dermis
Disfigurement or
defilement conflict
Sebaceous Glands
Conflict, that the
vagina is too dry
Penile, Glans Epidermis
Separation conflict
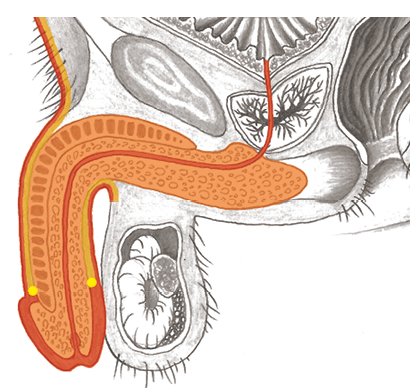
Urethra
Territorial-marking
conflict
Cavernous Body,
Subcutis,
Penile Frenulum
Local self-esteem
conflict

Genital herpes (herpes on the penis or testicles), inflammation
of the foreskin (posthitis), inflammation of the glans penis (balanitis), genital warts (Condylomata acuminata), pearly penile papules (hirsuties coronae glandis)
Chancroid (ulcus molle) in men
| Conflict-active | Conflict–active Degradation of epithelium, local loss of substance without pain = ulcer. |
|---|---|
| Repair phase | Restoration of the epithelial tissue with pain. |
| Therapy | Questions: see: p.319. Determine the conflicts and/or trigger(s) and, if possible, resolve them in real life if they are still active. |
Syphilis (lues)
Same SBS as above (see: p.319).
In CM, syphilis is seen as an infectious disease that advances in three stages (lues I-III).
As a matter of fact, the different lues stages are a collection of various SBS: pain in the head and limbs, swollen lymph nodes, hair loss, diseases of the stomach, liver, spleen, kidney, nerves, etc.
First-stage of syphilis symptoms: Painless ulcer on the outer genitals.
The tissue defects heal leaving hardened scars, which leads to the term “hard chancre”.
| Phase | Recurring–conflict, thus hard scars. |
|---|---|
| Therapy | Determine the conflict and/or trigger(s) and, if possible, resolve them in real life so that the persistent repair comes to an end. Questions: see: p.319. |

Penile melanoma
| Conflict | Disfigurement/attack/defilement, violation of integrity with regard to the penis. |
|---|---|
| Examples | ➜ A man finds sexual intercourse or certain sexual practices disgusting. ➜ Can also be experienced as a substitute for another person: a father is disgusted by the thought of the sexual practices of his homosexual son. ➜ Verbal attack on the penis or on a man‘s qualities as a lover. |
| Conflict-active | Conflict–active Cell proliferation local to the penis, growth of a melanoma. |
| Bio. function | Strengthening and thickening of the dermis so that the individual is protected better from disfigurement and deformation. |
| Repair phase | Caseating degradation of the melanoma. |
| Therapy | If the melanoma bleeds, the conflict is at least partially or temporarily resolved. If it grows imperceptibly, the conflict is active. Determine the conflict and conditioning and, if possible, resolve them. Hydrogen peroxide (H2O2) externally. If necessary, black salve or surgery. See also: chapter on skin, p. 341. |
Constriction of the foreskin (phimosis), short frenulum (frenulum breve)
| Conflict | Self-esteem conflict with relation to the foreskin or penis. Deeper cause: This symptom is usually worn by children on behalf of someone in the family to hide their masculinity. May not be or want to be a man. (For example, in the family, men are rejected or vilified). Similar conflict as with undescended testicles > often both symptoms occur at the same time. According to Frauenkron-Hoffmann: “Sex may not be pleasurable,” or a woman did not want to become pregnant. |
|---|---|
| Examples |  A grandmother and her daughter are single parents and resent men, blaming them for all their ills. The only son has a constriction of the foreskin. = Substitution conflict: To be loved he “holds his manhood back.“ (Archive B. Eybl) The father of a boy, who is affected by a constricted foreskin, lived in a family dominated by women: his father (the grandfather) died young and he had a domineering mother and dominant sister. = The boy carries the conflict for his father: “I am not allowed to be a man.” (Archive B. Eybl) A grandmother and her daughter are single parents and resent men, blaming them for all their ills. The only son has a constriction of the foreskin. = Substitution conflict: To be loved he “holds his manhood back.“ (Archive B. Eybl) The father of a boy, who is affected by a constricted foreskin, lived in a family dominated by women: his father (the grandfather) died young and he had a domineering mother and dominant sister. = The boy carries the conflict for his father: “I am not allowed to be a man.” (Archive B. Eybl) |
| Conflict-active | Conflict–active Degradation of cells from the collagenous and elastic fibers. Shrinkage due to a persistent conflict. > Constriction of the foreskin, shortening of the frenulum. |
| Bio. function | Reflecting the family energy outward to bring the issue to the attention of the family. |
| Repair phase | Repair phase Restoration, i.e., dilation of the foreskin without surgery is realistic if the conflict is resolved. |
| Questions | What is the manhood situation in the family? Do the women dominate? Where is the man? Does he influence family life? (Time, interest)? Does he lack the will to make his presence felt? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them. Man! Don’t be a coward! Mars meditation. Any surgery should be delayed as long as possible (is more tolerable later). This also increases the chances that the constriction of the foreskin repairs itself through conflict resolution. |
Peyronie‘s disease (induratio penis plastica), deformation of the penis (penis deviation)
| Conflict | Self-esteem conflict regarding the penis. |
|---|---|
| Examples | ➜ A late-developing boy is teased about his penis. ➜ A man has potency problems. ➜ A man suffers a painful and embarrassing kinking of the penis during sexual intercourse. |
| Conflict-active | Conflict–active Cell degradation from the cavernous bodies or other mesodermal part(s) of the penis. |
| Phase | Persistent repair or condition thereafter: restoration of the lost substance, possibly with excessive tissue growth; formation of flat, longish plaques; shrinkage; hardening; hour-glass-shaped constrictions; bottle-shaped narrowings in the area of the cavernous bodies, as well as penis deformations. |
| Bio. function | Strengthening of the affected structures. (Deformations indicate an unnaturally long conflict duration). |
| Note | According to the literature, patients with this disease pattern are at an increased risk of developing a prostate carcinoma. This is understandable from the point of view of the 5 Biological Laws of Nature, because a malformed penis brings ugly-genital conflicts along with it. |
| Questions | Did something happen during intercourse? A disparaging remark? Self-doubt? Why do I identify myself so strongly with my penis? (The fact of the matter is: For women, the penis is usually a secondary attribute at best. Being a good partner is more important to women). Is there a background of insecurity? What were my ancestors like? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them. OP if necessary. |
Inflammation of the prepuce II (inflammation of the smegma-producing glands)1
The smegma-producing glands lie on the inner side of the prepuce (foreskin) and secrete a whitish-yellow sebaceous substance (= lubricant and scent).
| Conflict | Chunk conflict (p. 15, 16), that the vagina one wants to penetrate is too dry. Problems during intercourse. |
|---|---|
| Examples | ➜ A man cannot enjoy sexual intercourse, because the vagina is too dry. ➜ Wanting to have sex with a woman, but not being allowed to. |
| Conflict-active | Conflict–active Increase in function, growth of the preputial glands and increased smegma production. |
| Bio. function | Increased lubrication facilitates the penis‘ entry into the vagina. |
| Repair phase | Tubercular-caseating degradation of excess cellular material, glandular inflammation of the prepuce, pain, swelling, reddening, probably often diagnosed as “inflammation of the foreskin.“ |
| Questions | Inflammation since when? (A related stress must have been resolved before this). First occurrence of symptoms? (No > find the first conflict). How was the first sexual contact? (Complications, disappointment)? Does sexuality have a negative connotation? (Something indecent, forbidden)? In a child: Did the father have difficulties during intercourse or problems related to sexuality? > Schedule/include parents in the therapy. |
| Therapy | The conflict is resolved. Support the healing. If it recurs, determine the conflict and/or trigger(s) and resolve them. Pay attention to the needs and desires of the woman, so that she also feels pleasure. If needed, use a lubricant. Colloidal silver internally and externally. If applicable, MMS (see p. 68) or antibiotics. See also Therapy p. 320. |
1 See Dr. Hamer, Charts p. 29
Painful erection (priapism)
Having multiple erections at night is normal. However, if they are painful or last for hours or days, this is called priapism.
Erotic feelings/sexual desire cause tension in the bulbospongiosus muscle via involuntary nerve impulses + hormones.
This also stops the backflow of venous blood from the penis. This is, biologically speaking, what leads to an erection. However, there is also a reason for this in the psyche:
| Conflict | According to Antje Scherret: Not being allowed to live out one’s sexual urges. Not getting your turn to be a man. |
|---|---|
| Example | A man has very strong urges. His wife at the time accuses him of being a “sex maniac.” She didn’t even like sleeping with him anymore = conflict of not being able to satisfy his urges. (“I’m not allowed to be horny.”) With the help of a 5BLN therapist he isolates his conflict. Then, in an EFT (Emotional Freedom Technique) session, he works on the belief, “I’m not allowed to be horny.” > After suffering from his priapism for years, he resolves it for good. (Archive Antje Scherret) |
| Conflict active | Tension in the smooth muscle portion of the bulbospongiosus (according to CM a striated muscle) > Persistent erection, pain, but able to urinate. |
| Repair/healing | Relaxation of the M. bulbospongiosus, backflow of the venous blood, healing softening of the member. |
| Bio function | Through the erection, the willingness and ability to mate is displayed openly – the individual gets his turn more quickly. |
| Questions | Symptoms since when? What changed shortly before this in my sex life? Pregnancy/birth of a child? (Wife doesn’t want to anymore) Partner gone? Divorce? Disappointing sexual contact? Rebukes/criticism? What conditioning lies behind it? Incidents related to this during childhood/puberty? What value did my male ancestors place on sexuality? Did this cause, e.g. fighting between parents in the past? Are you allowed to live out your sexuality? What belief structures may be playing a role? |
| Therapy | In CM, priapism is treated as an emergency because there is a fear of permanent damage. Whether that is justified needs to be decided on a case-by-case basis. Determine and resolve the belief structures and conditioning. |
Urethral stenosis (urethral stricture)
Mostly men are affected. Symptoms: weak or abnormal urine stream, difficulty urinating. The narrowing can cause residual urine to remain in the bladder, and in extreme cases urine can back up into the kidney (congested kidney).
Possible organic causes
• Injury caused by medical procedures (bladder catheter, cystoscopy, transurethal prostate surgery).
• Accidents (blunt injury to the crotch, e.g., due to falling on the crossbar of the bicycle or pelvic fracture).
• SBS of penile connective tissue: chronic devaluation conflict with regard to the penis or conflict of restricted masculinity. Scarring shrinkage of urethral connective tissue > urethral stenosis.
• SBS of the urethral mucosa: territorial marking conflict. Recurrent urethral inflammation (Urethritis) can lead to scarring and narrowing.
In both of the latter possibilities, the narrowing develops slowly/unnoticeably – in contrast to injury/accident.
In all of the above possibilities (yes, I think also in injury/accident), the following issue may be causative:
| Conflict | 1. Restricted masculinity, not allowed to be a man, disdain for masculinity (see foreskin constriction p. 321) 2. Territory marking conflict (see p. 282, 286). |
|---|---|
| Phase | Persistent (chronic) conflict. |
| Example | A 32-year-old man develops urethral and foreskin stenosis when he separates from his wife. His partner repeatedly belittles him as a man and finally no longer shows the slightest physical interest. He perceives this as disdain for his masculinity. The same issue arises with his next partner. (Archive B. Eybl) |
| Therapy | Find out and resolve the conflict, conditioning, and belief structures that caused it. In case of congenital urethral narrowing, it is necessary to look among one’s ancestors and treat accordingly. After dilatation surgery (dilation procedure), or incision surgery (urethrotomy procedure), new scars develop > moderate to long-term success. The difficult “open surgical reconstruction” is also risky. |
Potency disturbances (erectile dysfunction), reduced sex drive, male sterility
Possible causes
- Medication poisoning: Antihypertensives, psychopharmaceuticals, anti-cholesterol medications and many more particularly disturb the interaction of the autonomic nervous system > potency problems.
- Continuous-sympatheticotonia due to stress (one or more active conflicts or tracks): Sexual desire is pre-requisite to having an erection. Desire only comes during relaxation (vagotonia). See: p.13.
- Territory conflict or constellation: “Feminization“ due to the switch from the right “masculine“ side of the brain to the “feminine“ left side of the brain > potency problems or homosexuality (see pp. 151, 385).
- Testicles in persistent–conflict activity > reduced production of testosterone > reduced sex drive > potency problems (see: p.311).
- Self-esteem conflict in the conflict-active phase: reduced self-esteem, low energy levels > potency problems (see: p.353).
- Pituitary gland in the conflict-active phase: increased production of prolactin > potency problems (see: p.138).
Undersized penis (micropenis)
Possible causes (if not just imagined)
- Self-esteem conflict with regard to the penis in adolescence (CM: “idiopathic micropenis“). For example, derogatory notes about the appearance or size of the penis, possibly perceived vicariously = local self-esteem conflict: “I am not worth anything here!“ > persistent conflict activity – cell degradation or ceased growth in the mesenchymal penis tissue (see: p.353).
- Cerebral cortex constellation during adolescence > general developmental delay with postponed and inadequate development of the reproductive organs (see: p.385).
- Testicles in persistent repair during adolescence > reduced production of testosterone > underdevelopment of the male sex organs (see: p.311).
- Not enough growth hormone (somatotropin) during the growth phase (see: p.139).
- In the case of children, always think of the family: Possibly men are despised in the family or treated badly. In this case, the child is carrying the symptom for the family. “If I must be a man, then only with a small penis.“ If the adults change, reconcile > the child no longer needs to carry anything, can change naturally and return to “normal.”
All experience reports on the organ system „Penis and Urethra” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2025/10/21   A man has had recurring priapism almost every day for 20 years. Dissolving the belief with the help of EFT brings the solution and immediate and permanent cessation of the symptoms. | Priapism, Erectile dysfunction, permanent erection | ||||
2015/01/23   Severe bladder infection after acoustic borderline assault in dormitory. Two-phase very well comprehensible. |